Hickman Catheter
You have been given this leaflet because you need a Hickman Line inserting. This leaflet explains more about Hickman Line Insertion and answers some of the most frequently asked questions. If, after reading this leaflet, you have any questions or concerns, you should write them down and discuss them at your next appointment with your consultant, or the radiologist.
It is important that you understand the procedure, along with the potential benefits and risks before you agree to it.
What is a Hickman Line?
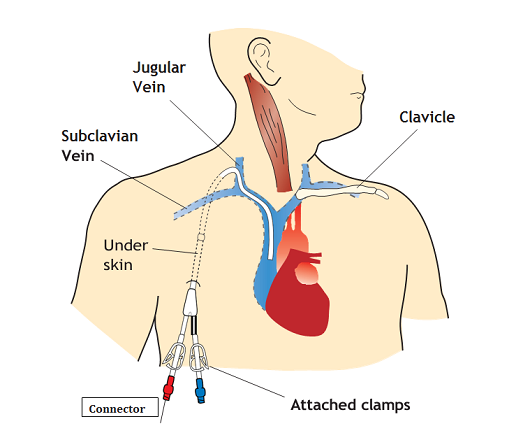
A Hickman line is a long thin tube made out of silicone. It is inserted so that one end lies in a large vein in the chest, with the other end lying outside of the body.
A portion of the line, between the two ends, is tunnelled under the skin of the upper chest. It has a cuff attached to it, which ultimately anchors the line in place and acts as a barrier to infection from the outside.
A single line can contain 1, 2 or 3 separate internal channels, each of which has an opening inside and outside the body. These provide a route for taking blood samples and giving intravenous (i.e. directly into a vein) treatment, and avoids the need to repeatedly puncture veins in the arms for this purpose. A clamp, and a connector to which a bung is attached, protect each of the openings on the outside of the body.
Hickman lines are used if it is thought your treatment is required for more than a couple of weeks. The type of line required is determined by your treatment. The duration of your treatment will determine how long the line is left in for. Care of the line is very important (other leaflets deal specifically with this). Your doctors and nurses will be able to give you further help and guidance if required.
How is it inserted?
Hickman lines are inserted by specialist doctors (radiologists) or trained radiographers in the X-ray department, using ultrasound and x-rays as guidance. The line is put in through the jugular vein at the bottom of the neck, or the subclavian vein below the collar-bone.
You will be asked to lie on your back on the X-ray table. You will be connected to monitoring equipment to check your heart tracing, blood pressure and blood oxygen levels.
It is very important to insert Hickman lines under sterile conditions to avoid infection. Hair on the skin at the entrance or exit sites may be removed. The radiologist will put on a sterile gown, theatre cap and mask, and you may need to wear a theatre cap also. The skin on your chest and neck is cleaned with antiseptic and you will then be covered in sterile towels.
Local anaesthetic is used to numb the skin over the vein (the ‘entrance site’) and a point lower down the front chest wall (the ‘exit site’), as well as the skin in between (which will form the tunnel).
A small incision is made at the entrance and exit sites. The vein is then punctured with a needle. One end of a special wire is passed through the needle into the vein. The other end of the wire remains outside of the body.
The Hickman line is tunnelled under the skin from the exit site to the entrance site. Your line is then measured and cut, to fit the length of your body’s vein.
A short tube (sheath) is placed over the wire and into the vein.
The wire is then removed and the free end of the Hickman line is placed through the sheath.
The position of line is adjusted until it is satisfactory. The line is secured at the exit site with a stitch. Another stitch is used to close the small incision at the entry site. A dressing is placed over these.
The Hickman line is flushed to ensure that there is no clotted blood with in it and it is then clamped off. The line is taped to the chest in a loop.
The procedure takes 30-45 minutes.
What happens before the procedure?
Generally, little preparation is required. There are no requirements to starve before insertion. If you are taking warfarin or other blood-thinning treatment, you should tell your doctor, as it may be necessary to alter your dosage beforehand. You should also tell your doctor if you have any allergies.
We must obtain your consent for any procedure or treatment beforehand. Staff will explain all the risks, benefits and alternatives before they ask for your consent. If you are unsure about any aspect of the procedure or treatment proposed, please do not hesitate to ask for more information.
Will it hurt?
Local anaesthetic may sting when it is first injected, but this wears off after a few seconds. The anaesthetic should remove any sharp sensations, but you may still be aware of some pressure on the skin during the procedure, particularly if working at the bottom of the neck. Most people tolerate this well, although it feels slightly strange.
Occasionally, people find it more uncomfortable and if that is the case, please let a member of staff know.
What happens afterwards?
If you are an inpatient, you should be well enough to return to the ward in the same way you came to the X-ray department. If you attend as an outpatient, you may be asked to remain in the department for an hour or so for routine observation, before being discharged.
The Hickman line can be used immediately following insertion.
Care must be taken not to tug on the line, particularly in the first 2 – 3 weeks following insertion, as the stitches holding it in cannot be tied too tightly (else they may block the line’s internal channels).
The entrance stitch is removed at 7-10 days and the exit stitch at 20-21 days. If you are at home the district or practice nurse will remove this.
Further information on safety, care of your Hickman line and troubleshooting is given in other leaflets which you will be provided with. See booklet “About your Hickman Line”.
Are there any risks or complications associated with insertion?
Hickman line insertion is a very common procedure. It is generally very safe, because of the use of ultrasound and x-ray machines to guide the person putting the line in.
However, complications do occasionally occur.
You may experience some bruising related to the insertion site, which usually settles with time.
There is a small risk of puncturing the artery which runs close to the vein – this is usually apparent to the radiologist, and is treated by pressing on the artery for a few minutes. It is very rare for any further treatment to be required.
The vein also lies close to the surface of the lung, and it is remotely possible that the lung could be punctured during Hickman line insertion. If this unlikely event were to occur, you might start to experience some shortness of breath and/or chest pain. If a punctured lung were to occur, a small drainage tube may need to be inserted into the chest, to allow the air leaking from the lung to escape.
Finally, the heart rhythm can occasionally be altered by the presence of a wire in the vein. Your heart tracing will be monitored during the procedure for this complication, and very rarely is any treatment required, other than to adjust the position of the wire.
Despite these potential risks, the vast majority of patients experience no problems whatsoever, and Hickman line insertion is a very safe and well tolerated procedure.
What else do I need to know?
Proper care of the Hickman line is very important after it has been inserted, particularly to stop it becoming infected or being pulled out. The medical and nursing staff should be able to help and advise you regarding your Hickman line, and other leaflets are available, dealing with these issues in more depth. See booklet “About your Hickman Line”.
What if I think there is something wrong when I get home?
If you think there is something wrong when you get home, you should contact the ward from which you were discharged or the angiography suite. If your problem is an emergency then please contact the Accident and Emergency Department.
Disclaimer: All rights reserved to the owner of the content. We are using it just for educational purpose.